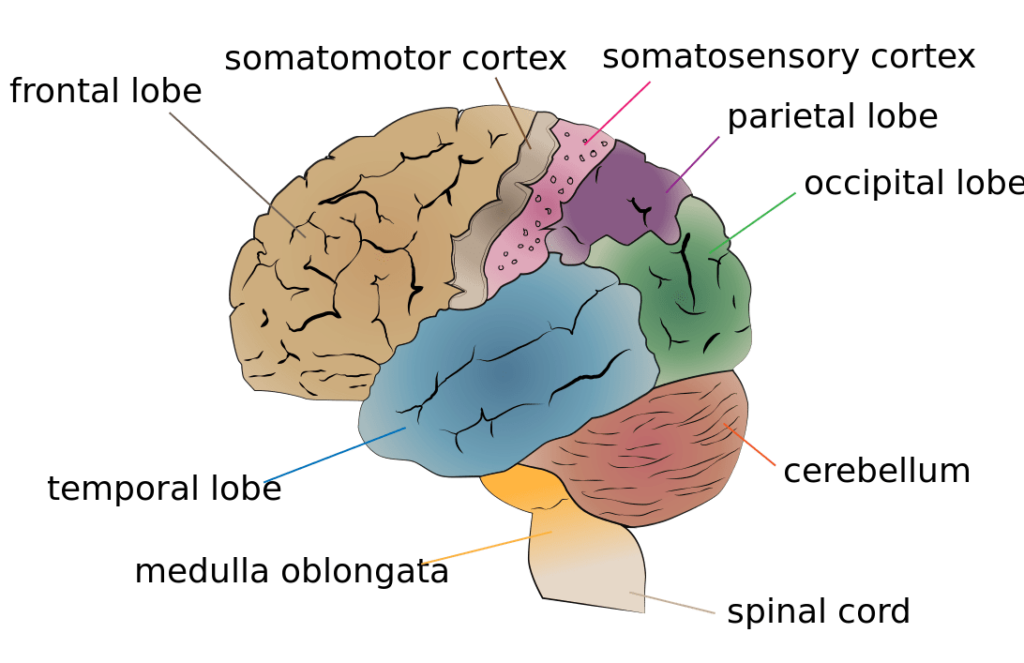

The cerebellum is largely responsible for coordinating the unconscious aspects of proprioception.
Proprioception (/ˌproʊprioʊˈsɛpʃən, -priə-/ PRO-pree-o-SEP-shən), from Latin proprius, meaning “one’s own”, “individual”, and capio, capere, to take or grasp, is the sense of the relative position of one’s own parts of the body and strength of effort being employed in movement.
In humans, it is provided by proprioceptors (muscle spindles) in skeletal striated muscles and tendons (Golgi tendon organ) and the fibrous capsules in joints. It is distinguished from exteroception, by which one perceives the outside world, and interoception, by which one perceives pain, hunger, etc., and the movement of internal organs.
The brain integrates information from proprioception and from the vestibular system into its overall sense of body position, movement, and acceleration. The word kinesthesia or kinæsthesia (kinesthetic sense) strictly means movement sense, but has been used inconsistently to refer either to proprioception alone or to the brain’s integration of proprioceptive and vestibular inputs.
Proprioception has also been described in other animals such as vertebrates, and in some invertebrates such as arthropods. More recently proprioception has also been described in flowering land plants (angiosperms).
History of Study
The position-movement sensation was originally described in 1557 by Julius Caesar Scaliger as a “sense of locomotion”. Much later, in 1826, Charles Bell expounded the idea of a “muscle sense”, which is credited as one of the first descriptions of physiologic feedback mechanisms. Bell’s idea was that commands are carried from the brain to the muscles, and that reports on the muscle’s condition would be sent in the reverse direction. In 1847 the London neurologist Robert Todd highlighted important differences in the anterolateral and posterior columns of the spinal cord, and suggested that the latter were involved in the coordination of movement and balance.
At around the same time, Moritz Heinrich Romberg, a Berlin neurologist, was describing unsteadiness made worse by eye closure or darkness, now known as the eponymous Romberg’s sign, once synonymous with tabes dorsalis, that became recognised as common to all proprioceptive disorders of the legs. Later, in 1880, Henry Charlton Bastian suggested “kinaesthesia” instead of “muscle sense” on the basis that some of the afferent information (back to the brain) comes from other structures, including tendons, joints, and skin. In 1889, Alfred Goldscheider suggested a classification of kinaesthesia into three types: muscle, tendon, and articular sensitivity.
In 1906, Charles Scott Sherrington published a landmark work that introduced the terms “proprioception”, “interoception”, and “exteroception”. The “exteroceptors” are the organs that provide information originating outside the body, such as the eyes, ears, mouth, and skin. The interoceptors provide information about the internal organs, and the “proprioceptors” provide information about movement derived from muscular, tendon, and articular sources. Using Sherrington’s system, physiologists and anatomists search for specialised nerve endings that transmit mechanical data on joint capsule, tendon and muscle tension (such as Golgi tendon organs and muscle spindles), which play a large role in proprioception.
Primary endings of muscle spindles “respond to the size of a muscle length change and its speed” and “contribute both to the sense of limb position and movement”. Secondary endings of muscle spindles detect changes in muscle length, and thus supply information regarding only the sense of position. Essentially, muscle spindles are stretch receptors. It has been accepted that cutaneous receptors also contribute directly to proprioception by providing “accurate perceptual information about joint position and movement”, and this knowledge is combined with information from the muscle spindles.
Components
A major component of proprioception is joint position sense, which is determined by measuring the accuracy of joint–angle replication. Clinical aspects of joint position sense are measured in joint position matching tests that measure a subject’s ability to detect an externally imposed passive movement, or the ability to reposition a joint to a predetermined position. These involve an individual’s ability to perceive the position of a joint without the aid of vision. Often it is assumed that the ability of one of these aspects will be related to another; however, experimental evidence suggests there is no strong relation between these two aspects. This suggests that while these components may well be related in a cognitive manner, they may in fact be physiologically separate.
More recent work into the mechanism of ankle sprains suggests that the role of reflexes may be more limited due to their long latencies (even at the spinal cord level), as ankle sprain events occur in perhaps 100 ms or less. In accordance, a model has been proposed to include a ‘feedforward’ component of proprioception, whereby the subject will also have central information about the body’s position before attaining it.
Kinesthesia is a key component in muscle memory and hand-eye coordination, and training can improve this sense (see blind contour drawing). The ability to swing a golf club or to catch a ball requires a finely tuned sense of the position of the joints. This sense needs to become automatic through training to enable a person to concentrate on other aspects of performance, such as maintaining motivation or seeing where other people are.
Basis of Proprioceptive Sense
The initiation of proprioception is the activation of a proprioreceptor in the periphery. The proprioceptive sense is believed to be composed of information from sensory neurons located in the inner ear (motion and orientation) and in the stretch receptors located in the muscles and the joint-supporting ligaments (stance). There are specific nerve receptors for this form of perception termed “proprioreceptors”, just as there are specific receptors for pressure, light, temperature, sound, and other sensory experiences. Proprioreceptors are sometimes known as adequate stimuli receptors. TRPN, a member of the transient receptor potential family of ion channels, has been found to be responsible for proprioception in fruit flies, nematode worms, African clawed frogs, and zebrafish. Piezo2, a nonselective cation channel, has been shown to underlie the mechanosensitivity of proprioceptors in mice. The channel mediating human proprioceptive mechanosensation has yet to be discovered.
Proprioception of the head stems from the muscles innervated by the trigeminal nerve, where the GSA fibers pass without synapsing in the Gasserian ganglion (first-order sensory neuron), reaching the mesencephalic tract and the mesencephalic nucleus of trigeminal nerve.
Although it was known that finger kinesthesia relies on skin sensation, recent research has found that kinesthesia-based haptic perception relies strongly on the forces experienced during touch. This research allows the creation of “virtual”, illusory haptic shapes with different perceived qualities.
Conscious and non-conscious proprioception
In humans, a distinction is made between conscious proprioception and non-conscious proprioception:
- Conscious proprioception is communicated by the posterior column-medial lemniscus pathway to the cerebrum.
- Non-conscious proprioception is communicated primarily via the dorsal spinocerebellar tract and ventral spinocerebellar tract, to the cerebellum.
- A non-conscious reaction is seen in the human proprioceptive reflex, or righting reflex—in the event that the body tilts in any direction, the person will cock their head back to level the eyes against the horizon. This is seen even in infants as soon as they gain control of their neck muscles. This control comes from the cerebellum, the part of the brain affecting balance.
Applications
Field sobriety test
Proprioception is tested by American police officers using the field sobriety test to check for alcohol intoxication. The subject is required to touch his or her nose with eyes closed; people with normal proprioception may make an error of no more than 20 millimeters, while people suffering from impaired proprioception (a symptom of moderate to severe alcohol intoxication) fail this test due to difficulty locating their limbs in space relative to their noses.
Diagnosis
There are several relatively specific tests of the subject’s ability to proprioceive. These tests are used in the diagnosis of neurological disorders. They include the visual and tactile placing reflexes.
Learning new skills
Proprioception is what allows someone to learn to walk in complete darkness without losing balance. During the learning of any new skill, sport, or art, it is usually necessary to become familiar with some proprioceptive tasks specific to that activity. Without the appropriate integration of proprioceptive input, an artist would not be able to brush paint onto a canvas without looking at the hand as it moved the brush over the canvas; it would be impossible to drive an automobile because a motorist would not be able to steer or use the pedals while looking at the road ahead; a person could not touch type or perform ballet; and people would not even be able to walk without watching where they put their feet.
Oliver Sacks has reported the case of a young woman who lost her proprioception due to a viral infection of her spinal cord. At first she could not move properly at all or even control her tone of voice (as voice modulation is primarily proprioceptive). Later she relearned by using her sight (watching her feet) and inner ear only for movement while using hearing to judge voice modulation. She eventually acquired a stiff and slow movement and nearly normal speech, which is believed to be the best possible in the absence of this sense. She could not judge effort involved in picking up objects and would grip them painfully to be sure she did not drop them.
Training
The proprioceptive sense can be sharpened through study of many disciplines. Examples are the Feldenkrais method and the Alexander Technique. Juggling trains reaction time, spatial location, and efficient movement. Standing on a wobble board or balance board is often used to retrain or increase proprioception abilities, particularly as physical therapy for ankle or knee injuries. Slacklining is another method to increase proprioception.
Standing on one leg (stork standing) and various other body-position challenges are also used in such disciplines as Yoga, Wing Chun and T’ai Chi Ch’uan. Also, the vestibular system of the inner ear, vision and proprioception are the main three requirements for balance. Moreover, there are specific devices designed for proprioception training, such as the exercise ball, which works on balancing the abdominal and back muscles.
Joint position matching
“Joint position matching” is an established protocol for measuring proprioception, and joint position sense specifically, without the aid of visual or vestibular information. During such tasks, individuals are blindfolded while a joint is moved to a specific angle for a given period of time, returned to neutral, and the subjects are asked to replicate the specified angle. Measured by constant and absolute errors, ability to accurately identify joint angles over a series of conditions is the most accurate means of determining proprioceptive acuity in isolation to date.
Recent investigations have shown that hand dominance, participant age, active versus passive matching, and presentation time of the angle can all affect performance on joint position matching tasks. Joint position matching has been used in clinical settings in both the upper and lower extremities.
Impairment
Temporary loss or impairment of proprioception may happen periodically during growth, mostly during adolescence. Growth that might also influence this would be large increases or drops in bodyweight/size due to fluctuations of fat (liposuction, rapid fat loss or gain) and/or muscle content (bodybuilding, anabolic steroids, catabolisis/starvation). It can also occur in those that gain new levels of flexibility, stretching, and contortion. A limb’s being in a new range of motion never experienced (or at least, not for a long time since youth perhaps) can disrupt one’s sense of location of that limb. Possible experiences include suddenly feeling that feet or legs are missing from one’s mental self-image; needing to look down at one’s limbs to be sure they are still there; and falling down while walking, especially when attention is focused upon something other than the act of walking.
Proprioception is occasionally impaired spontaneously, especially when one is tired. Similar effects can be felt during the hypnagogic state of consciousness, during the onset of sleep. One’s body may feel too large or too small, or parts of the body may feel distorted in size. Similar effects can sometimes occur during epilepsy or migraine auras. These effects are presumed to arise from abnormal stimulation of the part of the parietal cortex of the brain involved with integrating information from different parts of the body.
Proprioceptive illusions can also be induced, such as the Pinocchio illusion.
The proprioceptive sense is often unnoticed because humans will adapt to a continuously present stimulus; this is called habituation, desensitization, or adaptation. The effect is that proprioceptive sensory impressions disappear, just as a scent can disappear over time. One practical advantage of this is that unnoticed actions or sensation continue in the background while an individual’s attention can move to another concern. The Alexander Technique addresses these unconscious elements by bringing attention to them and practicing a new movement with focus on how it feels to move in the new way.
People who have a limb amputated may still have a confused sense of that limb’s existence on their body, known as phantom limb syndrome. Phantom sensations can occur as passive proprioceptive sensations of the limb’s presence, or more active sensations such as perceived movement, pressure, pain, itching, or temperature. There are a variety of theories concerning the etiology of phantom limb sensations and experience. One is the concept of “proprioceptive memory”, which argues that the brain retains a memory of specific limb positions and that after amputation there is a conflict between the visual system, which literally sees that the limb is missing, and the memory system which remembers the limb as a functioning part of the body. Phantom sensations and phantom pain may also occur after the removal of body parts other than the limbs, such as after amputation of the breast, extraction of a tooth (phantom tooth pain), or removal of an eye (phantom eye syndrome).
Temporary impairment of proprioception has also been known to occur from an overdose of vitamin B6 (pyridoxine and pyridoxamine). Most of the impaired function returns to normal shortly after the amount of the vitamin in the body returns to a level that is closer to that of the physiological norm. Impairment can also be caused by cytotoxic factors such as chemotherapy.
It has been proposed that even common tinnitus and the attendant hearing frequency-gaps masked by the perceived sounds may cause erroneous proprioceptive information to the balance and comprehension centers of the brain, precipitating mild confusion.
Proprioception is permanently impaired in patients that suffer from joint hypermobility or Ehlers-Danlos Syndrome (a genetic condition that results in weak connective tissue throughout the body). It can also be permanently impaired from viral infections as reported by Sacks. The catastrophic effect of major proprioceptive loss is reviewed by Robles-De-La-Torre (2006). There is also some evidence that proprioception is impaired in autism spectrum disorders such as Asperger Syndrome.
Proprioception is also permanently impaired in physiological aging (presbypropria).
Proprioception in plants
Terrestrial plants control the orientation of their primary growth through the sensing of several vectorial stimuli such as the light gradient or the gravitational acceleration. This control has been called tropism. However, a quantitative study of shoot gravitropism demonstrated that, when a plant is tilted, it cannot recover a steady erected posture under the sole driving of the sensing of its angular deflection versus gravity. An additional control through the continuous sensing of its curvature by the organ and the subsequent driving an active straightening process are required. Being a sensing by the plant of the relative configuration of its parts, it has been called proprioception. This dual sensing and control by gravisensing and proprioception has been formalized into a unifying mathematical model simulating the complete driving of the gravitropic movement. This model has been validated on 11 species sampling the phylogeny of land angiosperms, and on organs of very contrasted sizes, ranging from the small germination of wheat (coleoptile) to the trunk of poplar trees. This model also shows that the entire gravitropic dynamics is controlled by a single dimensionless number called the “Balance Number”, and defined as the ratio between the sensitivity to the inclination angle versus gravity and the proprioceptive sensitivity. This model has been extended to account for the effects of the passive bending of the organ under its self-weight, suggesting that proprioception is active even in very compliant stems, although they may not be able to efficiently straighten depending on their elastic deformation under the gravitational pull. Further studies have shown that the cellular mechanism of proprioception in plants involves myosin and actin, and seems to occur in specialized cells. Proprioception was then found to be involved in other tropisms and to be central also to the control of nutation.
These results change the view we have on plant sensitivity. They are also providing concepts and tools for the breeding of crops that are resilient to lodging, and of trees with straight trunks and homogeneous wood quality.
The discovery of proprioception in plants has generated an interest in the popular science and generalist media. This is because this discovery questions a long-lasting a priori that we have on plants. In some cases this has led to a shift between proprioception and self-awareness or self-consciousness. There is no scientific ground for such a semantic shift. Indeed even in animals, proprioception can be unconscious; so it is thought to be in plants.